|
|
Aortic Stenosis
General Considerations
- Most often as result of degeneration of bicuspid aortic valve
- Less commonly rheumatic heart disease or secondary to degeneration
of a tricuspid aortic valve in person > 65
Location
- Supravalvular
- Uncommon
- Associated with William’s Syndrome
- Hypercalcemia
- Elfin facies
- Pulmonary stenoses
- Hypoplasia of aorta
- Stenoses in
- Renal, celiac, superior mesenteric arteries
- Valvular
- Most common
- Either congenital (from a bicuspid aortic valve) or acquired
- Bicuspid aortic valve is the most common congenital cardiac anomaly
- Subvalvular
- Associated with
- Hypoplastic left heart syndrome
- Idiopathic Hypertrophic Subaortic Stenosis
- Hypertrophic cardiomyopathy
- Subaortic fibrous membrane
Types
- Congenital aortic stenosis (more common)
- Most frequent congenital heart disease associated with
intra-uterine growth retardation (IUGR)
- Subvalvular (30%)
- Valvular (70%)
- Degeneration of bicuspid valve
- Supravalvular
- Acquired aortic stenosis
- Rheumatic valvulitis
- Almost invariably associated with mitral valve disease
- Fibrocalcific senile aortic stenosis
Clinical Findings
- Asymptomatic for many years
- Classical triad
- Angina
- Syncope
- Shortness of breath (heart failure)
- Systolic ejection murmur
- Carotid pulsus parvus et tardus
- Diminished aortic component of 2nd heart sound
- Sudden death in severe stenosis after exercise
- Diminished flow in coronary arteries causes ventricular dysrhythmias
and fibrillation
- Decompensation leads to left ventricular dilatation and pulmonary
venous congestion
Imaging Findings
- In older children or young adults
- Prominent ascending aorta
- Poststenotic dilatation of ascending aorta
- Left ventricular heart configuration
- Normal-sized or enlarged left ventricle
- Concentric hypertrophy of left ventricle produces a relatively small
left ventricular chamber with thick walls
- Heart size is frequently normal
- In adults >30 years
- Prominent ascending aorta
- Poststenotic dilatation of ascending aorta
- Calcification of aortic valve (best seen on RAO)
- In females, usually indicates hemodynamically significant aortic stenosis
- Calcification of the valve usually indicates a gradient across
valve of > 50mm Hg
- Calcification begins in bicuspid and rheumatic valve in 4th decade
but not until > 65 in tricuspid
- DDx
- Calcification of aortic annulus in elderly
- Calcified coronary artery ostium (thickened cusp echoes only in diastole)
- Normal to enlarged left ventricle
Echocardiographic findings
- Thickened and calcified aortic valve with multiple dense cusp echoes
throughout cardiac cycle
- Right > non-coronary > left coronary cusp
- Decreased separation of leaflets in systole with reduced opening orifice
- (13-14 mm = mild AS; 8-12 mm = moderate AS; <8 mm = severe AS)
- ± Doming in systole
- Dilated aortic root
- Increased thickness of LV wall (= concentric LV hypertrophy)
- Hyperdynamic contraction of LV (in compensated state)
- Decreased mitral EF slope (reduced LV compliance)
- LA enlargement
- Increased aortic valve gradient (Doppler)
- Decreased aortic valve area (unreliable)
Angiographic findings
- Simultaneous LV and aortic pressures recordings yield valve gradients from left heart
catheterization
- Angiographic technique uses standard RAO left ventriculogram and an aortogram
using a 40° LAO projection
- A non-calcified, bicuspid valve reveals thickening and doming of the valve leaflets
in systole
- A jet of non-opacified blood is visible through stenotic valve
- Congenitally bicuspid valves still usually have three aortic sinuses with one large
non-coronary sinus equal in size to the other two
- Calcification begins in the bicuspid and rheumatic valve in the 4th decade
but not until >65 in tricuspid
- In rheumatic disease, the aortic valve commissures usually fuse whereas they
do not in the degenerated tricuspid valve
Differentiating Causes of Aortic Stenosis
| Etiology/Findings |
Calcification |
Other clues |
| Congenital Bicuspid Valve |
30’s |
Jet effect on aortogram |
| Degeneration of Tricuspid Valve |
> 65 |
Coronary artery ca++
Commissures don’t fuse |
| Rheumatic dz in Tricuspid Valve |
30’s here; teens in 3rd
world countries |
MS or MR almost always present;
commissures fuse |
Valve areas
Normal |
Mild |
Severe |
Critical |
2.6-3.5cm2 |
1.3-1.7 |
1.0 |
0.5 |


Aortic Stenosis. Top: Axial CT scan through heart demonstrates a heavily
calcified aortic valve (white arrow).
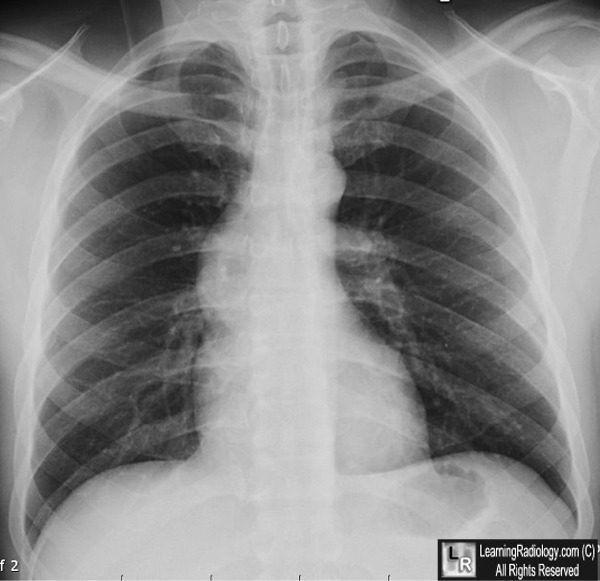
Bottom: Frontal chest radiograph in
another patient with aortic stenosis shows a dilated
ascending
aorta (white arrow) that abnormally projects farther
to the right than the right heart border.
This is caused by
post-stenotic dilatation of the aorta.
For these same photos without the arrows, click here and here
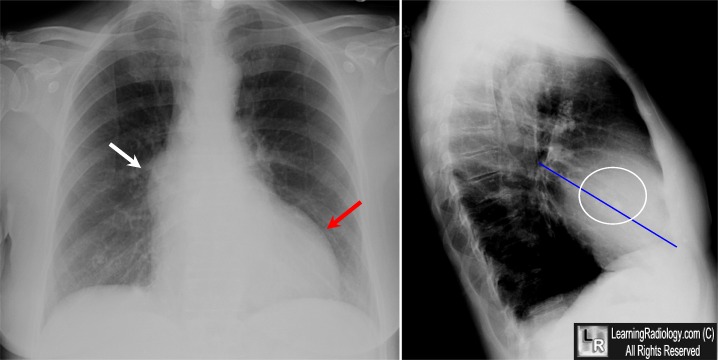
Aortic Stenosis. Frontal radiograph on left demonstrates isolated enlargement of the ascending aorta
(white arrow). The left ventricle is enlarged (red arrow) and the heart is mildly enlarged overall. The lateral view on the right demonstrates calcifications in the region of the aortic valve leaflets (circle). generally, the aortic valve lies above a line drawn from the carina to the junction of the diaphragm with the anterior chest wall. The mitral valve lies below the line.
For more information, click on the link if you see this icon 
|
|
|

{kind=link}
{kind=link}